

V体育安卓版 - PURPOSE
This phase I/II study evaluated tremelimumab (anticytotoxic T-lymphocyte–associated antigen-4 monoclonal antibody) and durvalumab (antiprogrammed death ligand-1 monoclonal antibody) as monotherapies and in combination for patients with unresectable hepatocellular carcinoma (HCC), including a novel regimen featuring a single, priming dose of tremelimumab (ClinicalTrials VSports注册入口. gov identifier: NCT02519348).
PATIENTS AND METHODS
Patients with HCC who had progressed on, were intolerant to, or refused sorafenib were randomly assigned to receive T300 + D (tremelimumab 300 mg plus durvalumab 1,500 mg [one dose each during the first cycle] followed by durvalumab 1,500 mg once every 4 weeks), durvalumab monotherapy (1,500 mg once every 4 weeks), tremelimumab monotherapy (750 mg once every 4 weeks [seven doses] and then once every 12 weeks), or T75 + D (tremelimumab 75 mg once every 4 weeks plus durvalumab 1,500 mg once every 4 weeks [four doses] followed by durvalumab 1,500 mg once every 4 weeks). Safety was the primary end point. Secondary end points included objective response rate (ORR) by Response Evaluation Criteria in Solid Tumors v1. 1 and overall survival; exploratory end points included circulating lymphocyte profiles V体育官网入口.
"V体育安卓版" RESULTS
A total of 332 patients were enrolled (T300 + D, n = 75; durvalumab, n = 104; tremelimumab, n = 69; and T75 + D, n = 84). Tolerability was acceptable across arms, with grade ≥ 3 treatment-related adverse events occurring in 37. 8%, 20. 8%, 43. 5%, and 24. 4%, respectively VSports在线直播. Confirmed ORRs (95% CI) were 24. 0% (14. 9 to 35. 3), 10. 6% (5. 4 to 18. 1), 7. 2% (2. 4 to 16. 1), and 9. 5% (4. 2 to 17. 9), respectively. An early expansion of CD8+ lymphocytes was associated with response across arms, with highest proliferating CD8+ lymphocyte levels occurring in the T300 + D arm. The median (95% CI) overall survival was 18. 7 (10. 8 to 27. 3), 13. 6 (8. 7 to 17. 6), 15. 1 (11. 3 to 20. 5), and 11. 3 (8. 4 to 15. 0) months in the T300 + D, durvalumab, tremelimumab, and T75 + D arms, respectively.
CONCLUSION
All regimens were found to be tolerable and clinically active; however, the T300 + D regimen demonstrated the most encouraging benefit-risk profile V体育2025版. The unique pharmacodynamic activity and association with ORR of the T300 + D regimen further support its continued evaluation in HCC.
"V体育平台登录" INTRODUCTION
Despite advances in treatment for unresectable hepatocellular carcinoma (uHCC), few patients achieve durable benefit and long-term survival rates remain poor. 1-4 An immune-suppressed tumor microenvironment in hepatocellular carcinoma (HCC), mediated in part by activated immune checkpoint signaling pathways, contributes to therapeutic resistance5 and provides the rationale to evaluate immunotherapy in this difficult cancer VSports. Programmed cell death receptor-1 and ligand-1 (PD-1/PD-L1) and cytotoxic T-lymphocyte–associated antigen-4 (CTLA-4) operate via complementary immunosuppressive signaling pathways,6 and a combination regimen designed to inhibit both pathways may improve outcomes in patients with uHCC.
CONTEXT
Key Objective
Patients with unresectable hepatocellular carcinoma have a poor prognosis. Immune checkpoint inhibitors (programmed cell death ligand-1 [PDL-1]/PD-L1; cytotoxic T-lymphocyte–associated antigen-4 [CTLA-4]) have shown promise, but are currently insufficient as single agents and, in the case of anti–CTLA-4, can be accompanied by challenging toxicities. We hypothesized that combination of a single, priming dose of tremelimumab (anti-CTLA-4) and durvalumab (anti-PDL1) every 4 weeks (T300 + D regimen) may provide the benefit of tremelimumab combination therapy while minimizing associated toxicity VSports app下载.
Knowledge Generated
The T300 + D regimen showed reduced toxicity compared with other tremelimumab-containing regimens and the highest efficacy compared with durvalumab and tremelimumab as monotherapy or in combination. T300 + D also stimulated CD8+ T-cell production, enhancing response and efficacy V体育官网.
Relevance
The T300 + D regimen displayed the most encouraging benefit-risk profile. These findings suggest that a single dose of tremelimumab may be sufficient to activate the tumor-fighting potential of the immune system. Both T300 + D and durvalumab monotherapy are being evaluated in the HIMALAYA study.
In solid tumors, combination regimens incorporating anti-CTLA-4 with anti-PD-L1 agents are associated with improved radiologic response and survival compared with monotherapies alone. Combinations incorporating higher doses of anti-CTLA-4 improved efficacy but were also associated with increased anti-CTLA-4 dose-dependent toxicity.7-11 Collective evidence indicates that prolonged or multiple exposures to CTLA-4 inhibitors may not be required for effective antitumor responses. A single dose of the CTLA-4 inhibitor tremelimumab was sufficient to provide long-lasting responses in patients with melanoma.12,13 In a phase Ib study of tremelimumab combined with the PD-L1 inhibitor, durvalumab, an expansion of CD4+ and CD8+ T cells was observed after the initial tremelimumab dose.14 The increased T-cell count was not observed with repeat dosing and largely subsided after 15 days.14 Similar results were seen in patients with melanoma after treatment with ipilimumab (anti-CTLA-4) plus nivolumab (anti-PD-1).15 As CTLA-4–related toxicity is typically observed after repeat dosing,11 we evaluated whether a single, priming dose of tremelimumab in combination with durvalumab could limit toxicity while maintaining the pharmacodynamic effect with similar or improved efficacy versus monotherapies.
The combination of tremelimumab (75 mg intravenous [IV], once every 4 weeks for four cycles) and durvalumab (1,500 mg IV once every 4 weeks; T75 + D) showed promising safety and initial efficacy in uHCC in the previously reported phase I cohort of this study.16 Expansion to a phase II portion initially enrolled patients to receive tremelimumab and durvalumab as monotherapies and in combination (T75 + D). After emergence of pharmacodynamic data,14,15 a second combination regimen featuring a single, priming dose of tremelimumab (300 mg IV, cycle 1) combined with durvalumab (1,500 mg IV once every 4 weeks; termed T300 + D) was added. The study was then subsequently expanded to part 3 to comprehensively evaluate all four regimens to determine whether either of the combination regimens could improve efficacy over monotherapies and whether the single, priming dose of tremelimumab in T300 + D could minimize the toxicity that may accompany repeat anti-CTLA-4 dosing (Appendix Fig A1, online only).
PATIENTS AND METHODS
Study Design and Conduct
This open-label, phase I/II study was conducted at 19 sites in nine countries (ClinicalTrials.gov identifier: NCT02519348) according to the Declaration of Helsinki. All patients provided written informed consent. Protocol approval was obtained from institutional review boards or ethics committees at each site.
The study was conducted in four parts (Appendix Fig A1). Part 116 evaluated T75 + D for initial safety and efficacy gating. In part 2A (n = 115), patients were randomly assigned 1:1:1 (via an interactive response system) to receive durvalumab monotherapy (1,500 mg IV once every 4 weeks), tremelimumab monotherapy (750 mg IV every 4 weeks × 7 doses and then once every 12 weeks thereafter), or the T75 + D regimen. Patients were then allocated to part 2B (n = 10) to examine the safety of the T300 + D regimen. In part 3 (n = 207), patients were randomly assigned 2:2:1:2 across four randomized arms: T300 + D, durvalumab monotherapy, tremelimumab monotherapy, and T75 + D. See the Data Supplement (online only) for patient stratification factors and treatment discontinuation details.
Patients
Eligible patients (≥ 18 years or ≥ 20 years [Japan]) had uHCC confirmed by previous histologic diagnosis and/or by radiologic criteria17,18; all patients were required to provide a fresh or archival tumor tissue sample. Patients were immunotherapy-naïve; had progressed on, were intolerant to, or refused treatment with sorafenib; and had Child-Pugh Score class A and Eastern Cooperative Oncology Group performance status 0-1. Patients with hepatitis B virus or hepatitis C virus infection were permitted. Additional enrollment criteria and definitions for sorafenib intolerance are provided in the Data Supplement.
Assessments
The primary end point was safety. Adverse events (AEs) were monitored and graded by investigators using the National Cancer Institute Common Terminology Criteria for Adverse Events, v4.03. Treatment-related AEs (trAEs) were determined based on investigator assessment of relationship to treatment, and immune-mediated AEs (imAEs) were also assessed.
Response measurements were collected every 8 weeks (RECIST 1.1) and assessed locally by site investigators for treatment decisions and centrally by a blinded independent central review (BICR) radiologist. Secondary end points per BICR included objective response rate (ORR), duration of response (DoR), time to response, and progression-free survival (PFS), as well as overall survival (OS; per investigator assessment only). See the Data Supplement for biomarker assessments, including associated discriminant analyses.
Statistical Analyses
In part 2A, a sample size of 108 patients was estimated to yield approximately 12 patients per viral status cohort in the monotherapy arms, providing ≥ 72% probability of observing ≥ 1 AE in each cohort, assuming the incidence of 10%-15%. In part 3, an estimated total of 64 patients treated with durvalumab monotherapy would provide a 96% probability of observing ≥ 1 AE, assuming the incidence of 5%. The combined total estimated sample size was approximately 200.
Safety data were analyzed using descriptive statistics for patients who received ≥ 1 dose of study treatment. Efficacy outcomes were summarized by arm, including frequency and ORR; median and corresponding 95% CIs were estimated for OS, PFS, and DoR using the Kaplan-Meier method.
See the Data Supplement for biomarker methods.
RESULTS
Patients
As of February 28, 2020, 332 patients were enrolled in parts 2 and 3 (T300 + D, n = 75; durvalumab, n = 104; tremelimumab, n = 69; and T75 + D, n = 84; Fig 1). Patient demographics and baseline characteristics were generally balanced across groups (Table 1 and Data Supplement). Most patients had advanced HCC (ie, Barcelona Clinic Liver Cancer stage B or C) and Child-Pugh score A; 2.4% declined to B/7 between screening and random assignment or treatment. The majority progressed on (51.8%) or were intolerant to (15.4%) sorafenib. The median duration of previous sorafenib therapy was 3.9 months.
FIG 1.

CONSORT diagram of patient disposition in parts 2 and 3. AE, adverse event; D, durvalumab; HCC, hepatocellular carcinoma; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
TABLE 1.
Demographic and Clinical Characteristics of Patients With Unresectable Hepatocellular Carcinoma

Safety
The safety analysis included 326 patients from parts 2 and 3. The median (range) duration of exposure was 3.7 (0.8-27.1) months for T300 + D, 3.7 (0.7-34.3) months for durvalumab, 3.7 (0.9-31.2) months for tremelimumab, and 2.4 (0.6-31.4) months for T75 + D. trAEs and grade ≥ 3 trAEs were highest with tremelimumab (Table 2). For T300 + D, the most common trAEs were grade 1 or 2 cutaneous AEs. The most common grade ≥ 3 trAEs overall included increased aspartate aminotransferase, increased lipase, increased amylase, and diarrhea. However, these increased laboratory values were transient and/or asymptomatic. Serious trAEs were highest with tremelimumab monotherapy (24.6%); incidences were 17.6%, 10.9%, and 14.6% with T300 + D, durvalumab, and T75 + D, respectively. trAEs requiring systemic steroids were distributed across system organ class, and grade 3 or 4 rates were low overall. They were reported at higher frequency in the tremelimumab-containing arms (T300 + D: 24.3%, tremelimumab: 26.1%, and T75 + D: 24.4%) versus durvalumab (9.9%; Data Supplement). imAEs were also reported at a higher frequency in the tremelimumab-containing arms (T300 + D: 31.1%, T: 24.6%, T75 + D: 26.8%) versus the D arm (15.8%; Data Supplement). The frequencies of hepatic standardized MedDRA Query AEs were comparable across arms (Data Supplement), as was the frequency of hepatic standardized MedDRA Query AEs considered causally related by investigators (T300 + D: 28.4%, D: 18.8%, T: 18.8%, and T75 + D: 23.2%). AEs of hepatitis and hepatic failure were low for all arms (n = 1-2 per arm for each). One (1.4%), 4 (4.0%), 1 (1.4%), and 3 (3.7%) patients on T300 + D, D, T75 + D, and T, respectively, required steroids for hepatobiliary disorders (Data Supplement). An antidrug antibody (ADA) response to durvalumab was found in only one patient on study who was receiving T75 + D. ADA-positive responses for tremelimumab at any visit were identified in 7 (13%), 5 (16.1%), and 3 (7.3%) patients receiving T300 + D, tremelimumab, and T75 + D, respectively. Treatment-emergent ADA incidences were 7.4% (n = 4) with T300 + D, 16.1% (n = 5) with T, and 7.3% (n = 3) with T75 + D (Data Supplement).
TABLE 2.
Common trAEs (≥ 5% in Any Group)a

The most frequent reasons for treatment discontinuation were disease progression (210 [64.4%]) and AEs (34 [10.4%]). Discontinuation because of trAEs was similar across arms; 10.8%, 7.9%, 13.0%, and 6.1% discontinued T300 + D, durvalumab, tremelimumab, and T75 + D, respectively. Discontinuation because of imAEs was also similar across arms. Possible trAEs that led to death (grade 5 trAEs) occurred in one patient who received T300 + D (pneumonia), three patients who received durvalumab (pneumonitis, abnormal hepatic function, and hepatic failure), none who received tremelimumab, and one who received T75 + D (hepatic failure). Another patient in the T300 + D arm died from an unknown cause where relationship to treatment could not be determined by the investigator.
Efficacy
Efficacy analyses were performed for each treatment arm for parts 2A, 2B, and 3 combined, and for part 3 alone. Overall, the results were consistent between parts, and therefore, only the results of the combined data are presented here. See the Data Supplement for part 3 alone (Appendix Figs A2 and A3, online only; Data Supplement). The confirmed ORR by BICR was highest for T300 + D (24.0%; 95% CI, 14.9 to 35.3; Table 3). Confirmed complete responses were achieved by one patient receiving T300 + D and two receiving T75 + D. Median time to response was shortest with T300 + D (1.86 months) and tremelimumab (1.81 months). The median DoR was not reached with T300 + D and was 11.17 months, 23.95 months, and 13.21 months with durvalumab, tremelimumab, and T75 + D, respectively (Table 3). Responses occurred across PD-L1 and viral status subgroups (Appendix Fig A4, online only). One patient in each of the tremelimumab-containing arms had an initial ≥ 5% increase in tumor size from baseline at first scan, but subsequently achieved partial or complete responses (Appendix Fig A5, online only).
TABLE 3.
Response Outcomes

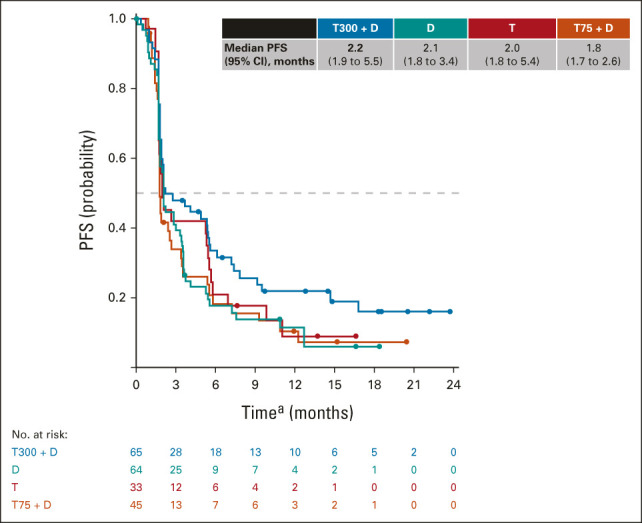
The median PFS (95% CI) was 2.17 (1.91 to 5.42) months with T300 + D, 2.07 (1.84 to 2.83) months with durvalumab, 2.69 (1.87 to 5.29) months with tremelimumab, and 1.87 (1.77 to 2.53) months with T75 + D (Appendix Fig A6, online only). The median (95% CI) OS was highest with T300 + D at 18.73 (10.78 to 27.27) months, followed by 15.11 (11.33 to 20.50) months with tremelimumab, 13.57 (8.74 to 17.64) months with durvalumab, and 11.30 (8.38 to 14.95) months with T75 + D (Fig 2). Analysis of OS and ORR by previous sorafenib/vascular endothelial growth factor receptor tyrosine kinase inhibitor exposure and viral status found that T300 + D was associated with the longest median OS independent of line of therapy (Data Supplement) and the highest ORR independent of viral etiology (Data Supplement). No differences in efficacy from the overall population were observed for any viral subgroup. Five (6.7%) and 3 (3.6%) patients were treated with T300 + D and T75 + D, respectively, beyond progression, per investigator assessment. After treatment completion, 42.7%, 35.6%, 31.9%, and 38.1% in the T300 + D, durvalumab, tremelimumab, and T75 + D arms, respectively, received subsequent therapy; most received systemic therapy (Data Supplement).
FIG 2.

Kaplan-Meier analysis of OS. aTime from random assignment (parts 2A and 3) or first dose (part 2B). bOne event observed at 27 months in the T300 + D arm. D, durvalumab; OS, overall survival; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
Biomarker Analyses
Baseline immune cell profiles were similar across all arms (Data Supplement). Quadratic discriminant analysis of 26 lymphocyte population values on day 15 revealed that patients were maximally discriminated by two discrete combinations of lymphocyte populations, canon-1 and canon-2, which were associated with CD4+ and CD8+ T cells, respectively. Patients receiving T300 + D exhibited the highest canon-2 scores (Fig 3A). Linear regression analysis revealed that canon-2 was predominantly associated with elevations in the Ki67+ subset of CD8+ T cells (Appendix Fig A7, online only). Response was associated with an expansion of these CD8+Ki67+ lymphocytes occurring early during treatment (day 15). The highest median counts were observed with T300 + D (Fig 3B, Appendix Fig A8, online only), consistent with the observation that T300 + D yielded the highest ORR (Table 3).
FIG 3.

Biomarker analysis of day 15 patient whole-blood samples. (A) Canonical score plot derived from quadratic discriminant analysis of 26 lymphocyte population values that identified two combinations of populations (canons) that best classify each patient into the assigned treatment arm. Canon 1 is composed of CD4+ T-cell populations and canon 2 of CD8+ T-cell populations. Percent misclassified: 1.7% (2 of 117); entropy R2: 0.92. (B) Analysis of patient CD8+ Ki67+ T-cell counts stratified by treatment arm and response. CR, complete response; D, durvalumab; PD, progressive disease; PR, partial response; SD, stable disease; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
DISCUSSION
This is the first randomized study in a predominantly second-line uHCC population who received PD-L1 or CTLA-4 inhibitors as monotherapies or combinations. Among regimens investigated, T300 + D provided the best benefit-risk profile.19-22 The toxicity profile for T300 + D was favorable when compared with other anti-CTLA-4/PD-1(L1) combinations23-25 and consistent with published monotherapies.19-22 Additionally, although durable responses occurred across arms, T300 + D demonstrated the greatest efficacy, including a confirmed ORR of 24%, median DoR that was not reached, and a median OS of 18.73 months. All treatment regimens were tolerable and had manageable safety profiles in the target patient population; no new safety signals were identified.
Previous data for nivolumab (1 mg/kg) and high-dose ipilimumab (3 mg/kg once every 3 weeks for four doses) combination followed by nivolumab monotherapy in uHCC (CheckMate-040) and other tumors23-25 resulted in the longest median OS, but are also associated with high rates of immune toxicity; in uHCC, more than 50% of patients in CheckMate-040 required systemic corticosteroids and the discontinuation rate because of trAEs was 22%.26,27 By contrast, trAEs requiring discontinuation in this study occurred in 6%-13% of patients across arms and were highest with tremelimumab. Moreover, incidence of trAEs requiring systemic steroids for the T300 + D regimen was 24.3%, and the safety profile appeared favorable; only 10.8% discontinued because of trAE. Furthermore, incidences of imAEs of hepatitis or hepatic failure were low for all arms (≤ 2 patients per arm).
ADA rates reported for other immunotherapies in uHCC are varied (28% with atezolizumab and 45%-56% with nivolumab, dose-dependent).28-31 Although ADAs associated with atezolizumab can affect clinical efficacy,30 the same has not been shown for nivolumab,28 despite the higher frequency. These results suggest that absolute ADA rates alone may not be predictive of an impact on clinical activity, and understanding the role of neutralizing antibodies as part of the ADA response could be critical. Here, durvalumab and tremelimumab had lower rates across all arms (≤ 2.3% and ≤ 16.1%, respectively). Although most occurrences of ADAs for tremelimumab were classified as persistently positive, > 90% were because a single ADA response was recorded at the final assessment. Overall, the full impact of ADAs on clinical efficacy for immunotherapies warrants further exploration.
Proliferative CD8+Ki67+ T-cell counts were associated with radiographic response regardless of treatment received but were highest after T300 + D, supporting the mechanism of enhanced immune activation. Moreover, the T-cell profile observed via quadratic discriminant analysis in patients treated with T300 + D was distinct from those treated with durvalumab monotherapy and T75 + D, which were similar. These data reflect results in non–small-cell lung cancer14 and other solid tumors,15 suggesting that combinations may not simply be additive but rather yield distinct expression profiles.32 In summary, favorable clinical outcomes with T300 + D, coupled with unique proliferative T-cell response, warrant further studies of this approach.
The tremelimumab monotherapy arm represents the first large cohort of patients with HCC to receive treatment with an anti-CTLA-4 monotherapy. Although ORR was lowest in this arm, median OS was the second longest and median DoR was prolonged (23.95 months). This suggests that tremelimumab alone is capable of driving sustained, durable responses and is consistent with existing data from patients treated with anti-CTLA-4 agents across multiple tumor types.26,33 The apparent disconnect between ORR and OS suggests that anti-CTLA-4 therapy can drive sustained or delayed immune-mediated effects for some patients with HCC, despite a lack of radiologic response. The disparity between OS and ORR may result from using RECIST 1.1, which does not account for different patterns of clinical response and progression.34,35 Increases in tumor size followed by reduction can occur with immunotherapies36; a phenomenon termed pseudoprogression.36-38 Although pseudoprogression with checkpoint inhibition is rare, there may be a broader potential for atypical patterns of response with CTLA-4 inhibition with or without PD-1/PD-L1 inhibition.39-43 Additionally, disease stabilization after initial progression has been documented for PD-1 inhibitors and is associated with prolonged survival.26
In this study, patients in tremelimumab-containing arms demonstrated cases of atypical patterns of response (Appendix Fig A4), indicating that early progression per conventional criteria does not always imply a poor survival prognosis and can confound PFS interpretation. The potential for anti-CTLA-4 agents to provide a survival benefit despite a lack of response per RECIST 1.1 may warrant treatment after initial progression and/or alternative means of assessing progression after immunotherapy, such as immune-related RECIST.36,44 Previous studies with other immunotherapies in HCC reported strong improvements in ORR evaluated using these other methods versus RECIST v1.1.34,45
Perhaps the most remarkable finding for immunotherapies is the capacity to provide durable, long-term survival, leading to substantial survival tails in the Kaplan-Meier OS curves associated with anti-CTLA-412,13 and anti-PD-1 agents.21,46,47 In Checkmate-067, both anti-CTLA-4 and anti-PD-1 agents were shown to drive the formation of the survival tail; however, the greatest benefit was observed when both were given in combination. Another key finding observed with immunotherapies is that the separation between the survival curves of checkpoint inhibitors and standard-of-care agents can be delayed,21,46,47 suggesting that longer periods of follow-up may be required to ascertain OS benefit when studying novel immunotherapy combinations like T300 + D.47,48 This may also complicate the comparison of OS in randomized controlled trials using the proportional risk methods.
A limitation of this study was the absence of a standard-of-care control. Although data from parts 2 and 3 were pooled, the four arms were not powered for direct comparison and between-arm comparisons were further confounded by the differences in start times, patient random assignment, and stratification factors between parts 2 and 3. At study initiation, a modified TNM staging approach including fibrosis and Child-Pugh scores was used, resulting in the under-reporting of Barcelona Clinic Liver Cancer scores in part 2A. Although most patients were enrolled after progressing on or intolerance to sorafenib, a subset in each arm refused sorafenib therapy and were treated as first line. This limitation was mitigated in part 3 where stratification included sorafenib status. Notably, ORRs were consistent regardless of sorafenib usage, suggesting that T300 + D provides the best all-around response benefit. Finally, the analysis of circulating lymphocytes was limited by the number of patients with accompanying evaluable tumor specimens and lack of paired on-treatment tumor specimens to evaluate changes in the tumor immune microenvironment. Baseline and on-treatment tumor analyses of immune microenvironment and PD-L1 expression are ongoing.
The treatment landscape for uHCC has evolved rapidly, with regulatory approval of atezolizumab plus bevacizumab in 2020.4 In addition, other immunotherapy-containing regimens are being evaluated, including combinations of immune checkpoint inhibitors with antiangiogenic agents lenvatinib (ClinicalTrials.gov identifier: NCT03517449) and cabozantinib (ClinicalTrials.gov identifier: NCT03755791), and nivolumab plus ipilimumab (ClinicalTrials.gov identifier: NCT04039607). With multiple new treatments likely to be available, T300 + D may offer distinct differentiating features beyond demonstration of durable objective responses and promising OS, including a favorable safety profile with a relatively low steroid requirement, rare ADA formation, and a single, priming dose of tremelimumab followed by monthly durvalumab administration schedule. Moreover, the absence of an antiangiogenic partner allows for treatment of patients who are contraindicated for antiangiogenics because of bleeding risks or comorbidities like cardiovascular disease.
In conclusion, the encouraging safety profile and clinical activity of a single priming dose of tremelimumab combined with durvalumab once every 4 weeks suggest that this regimen may provide improved safety and durable responses versus either agent alone or versus a combination (including a lower, repeated dose of tremelimumab) in patients with uHCC. The unique pharmacodynamic activity of the tremelimumab priming dose on proliferative T cells substantiates its clinical efficacy. The T300 + D regimen and durvalumab monotherapy are being evaluated versus sorafenib in the ongoing phase III HIMALAYA study (ClinicalTrials.gov identifier: NCT03298451).
ACKNOWLEDGMENT
The authors would like to thank the patients, their families and caregivers, and all investigators involved in this study. The authors would also like to thank the independent reviewers and readers of the images of this study. Medical writing support, which was in accordance with Good Publication Practice (GPP3) guidelines, was provided by Jubilee Stewart, PhD, and Lauren D. Van Wassenhove, PhD, of Parexel (Hackensack, NJ) and was funded by AstraZeneca.
Appendix (VSports)
FIG A1.

Study design for parts 1-3 (part 4 evaluated durvalumab plus bevacizumab in patients with first-line unresectable hepatocellular carcinoma and will be published separately). D, durvalumab; FSI, first subject in; LSI, last subject in; n, No. of enrolled patients; R, randomly assigned; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
"V体育安卓版" FIG A2.

Kaplan-Meier analysis of OS, part 3 only. aTime from random assignment. D, durvalumab; NR, no response; OS, overall survival; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
FIG A3.
Kaplan-Meier analysis of progression-free survival, part 3 only. aTime from random assignment. D, durvalumab; PFS, progression-free survival; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks [four doses] plus durvalumab 1,500 mg once every 4 weeks.
"VSports注册入口" FIG A4.

Target lesion response for (A) T300 + D (ORR = 24.0%), (B) durvalumab (ORR = 10.6%), (C) tremelimumab (ORR = 7.2%), and (D) T75 + D treatment cohorts (ORR = 9.5%) in parts 2 and 3. aPatients who achieved a response. D, durvalumab; HBV, hepatitis B virus; HCV, hepatitis C virus; M, PD-L1 status missing; ORR, overall response rate; PD-L1, programmed cell death ligand-1; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
FIG A5. (V体育平台登录)

Best response for target lesion from baseline. (A) T300 + D. (B) Durvalumab. (C) Tremelimumab. (D) T75 + D. CR, complete response; D, durvalumab; PD, progressive disease; PR, partial response; SD, stable disease; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
FIG A6.

Kaplan-Meier analysis of PFS, parts 2 and 3. aTime from random assignment (part 2A, 3) or first dose (part 2B). D, durvalumab; PFS, progression-free survival; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
FIG A7.

Correlation (correlation coefficient > 0.1) of lymphocyte population counts for all treatment arms combined with canon-1 or canon-2 scores. ((A) CD4+Ki67+ T cells. (B) CD8+Ki67+ T cells. (C) CD4+ICOS+ T cells. (D) CD4+HLA-DR+ T cells. (E) CD8+ICOS+ T cells. (F) CD4+ Tem cells. (G) CD4+ Tcm cells. (H) CD4+CD38+ T cells. HLA-DR, Human Leukocyte Antigen of the DR type; ICOS, inducible T cell costimulator; Tcm, central memory T cells; Tem, effector memory T cells.
FIG A8.

CD3+ CD8+ Ki67+ T-cell analysis of patient samples by response at day 1 and day 15. CR, complete response; D, durvalumab; PD, progressive disease; PR, partial response; SD, stable disease; T, tremelimumab; T300 + D, tremelimumab 300 mg plus durvalumab 1,500 mg for one dose each during the first cycle followed by durvalumab 1,500 mg once every 4 weeks; T75 + D, tremelimumab 75 mg once every 4 weeks (four doses) plus durvalumab 1,500 mg once every 4 weeks.
Robin Kate Kelley
Consulting or Advisory Role: Agios, AstraZeneca, Bristol Myers Squibb, Genentech/Roche, Merck, Gilead Sciences, Exact Sciences
Research Funding: Lilly, Exelixis, Novartis, Bristol Myers Squibb, MedImmune, Merck Sharp & Dohme, Agios, AstraZeneca, Adaptimmune, Taiho Pharmaceutical, Bayer, QED Therapeutics, EMD Serono, Partner Therapeutics, Genentech/Roche
Travel, Accommodations, Expenses: Ipsen
Bruno Sangro
Consulting or Advisory Role: Bristol Myers Squibb, AstraZeneca, Bayer, Adaptimmune, Sirtex Medical, BTG, Merck, H3 Biomedicine, Ipsen, Lilly, Roche/Genentech, Eisai, Incyte
Speakers' Bureau: Bristol Myers Squibb, Bayer, Sirtex Medical, Ipsen, Lilly, AstraZeneca, Eisai, Incyte, Roche
Research Funding: Bristol Myers Squibb, Sirtex Medical
Travel, Accommodations, Expenses: AstraZeneca, Bristol Myers Squibb, Sirtex Medical, Bayer
Other Relationship: Medscape, Target Pharmasolutions
William Harris
Consulting or Advisory Role: Neo Therma, Eisai, Exelixis, Bristol Myers Squibb, QED Therapeutics, Zymeworks
Research Funding: ArQule, Exelixis, Halozyme, Bristol Myers Squibb, MedImmune, Agios, Bayer, Merck, BTG
Travel, Accommodations, Expenses: Eisai
Masafumi Ikeda
Honoraria: Taiho Pharmaceutical, Bayer Yakuhin, Eisai, Lilly Japan, Dainippon Sumitomo Pharma, Teijin Pharma, EA Pharma, MSD, Mylan, Otsuka, Yakult Pharmaceutical, Servier, Astellas Pharma, Chugai Pharma, Takeda, AstraZeneca, Novartis, Bristol Myers Squibb
Consulting or Advisory Role: Bayer Yakuhin, Eisai, Novartis, Lilly Japan, Chugai Pharma, Micron, Ono Pharmaceutical, AstraZeneca, Servier, Takeda, GlaxoSmithKline, EMD Serono
Research Funding: Bayer Yakuhin, Yakult Pharmaceutical, Lilly Japan, Ono Pharmaceutical, Eisai, AstraZeneca, Chugai Pharma, Bristol Myers Squibb, ASLAN Pharmaceuticals, Novartis, MSD, J-Pharma, Takeda, Pfizer, Nobelpharma, Merck, Delta-Fly Pharma, Chiome Bioscience, Merus NV
Takuji Okusaka
Honoraria: Eisai, Ono Pharmaceutical, Taiho Pharmaceutical, Lilly, AstraZeneca, Chugai Pharma, Yakut Honsha, Daiichi Sankyo
Consulting or Advisory Role: Taiho Pharmaceutical, Dainippon Sumitomo Pharma, Bristol Myers Squibb, AstraZeneca, Eisai, Nihon Servier
Research Funding: Novartis, Eisai, Dainippon Sumitomo Pharma, Baxter, Lilly, Taiho Pharmaceutical, AstraZeneca, Chugai Pharma, Bristol Myers Squibb, MSD
Yoon-Koo Kang
Consulting or Advisory Role: DAE HWA Pharmaceutical, Bristol Myers Squibb, Zymeworks, ALX Oncology, Amgen, Novartis, Macrogenics, Surface Oncology, Blueprint Medicines
David W.-M. Tai
Honoraria: Bristol Myers Squibb, Eisai
Consulting or Advisory Role: Bristol Myers Squibb, Eisai
Speakers' Bureau: Ipsen, Bristol Myers Squibb, Eisai, Roche
Research Funding: Bristol Myers Squibb, Sirtex Medical, Novartis
Ho Yeong Lim
Honoraria: Bayer, Eisai, MSD Oncology, Bristol Myers Squibb/Medarex, AstraZeneca
Consulting or Advisory Role: Bayer, Eisai, Bristol Myers Squibb, AstraZeneca
Speakers' Bureau: Bayer
Thomas Yau
Honoraria: Bristol Myers Squibb, MSD Oncology, AstraZeneca
Consulting or Advisory Role: Bristol Myers Squibb
Wei-Peng Yong
Consulting or Advisory Role: AbbVie/Genentech, Amgen, Bristol Myers Squibb, Ipsen, Novartis, AstraZeneca
Speakers' Bureau: Lilly, Sanofi/Aventis, Taiho Pharmaceutical, Eisai, Bayer, MSD Oncology
Travel, Accommodations, Expenses: Pfizer
Ann-Lii Cheng
Honoraria: Bayer Yakuhin, AstraZeneca, Eisai, Genentech/Roche
Consulting or Advisory Role: Bristol Myers Squibb, Bayer Schering Pharma, Eisai, Ono Pharmaceutical, AstraZeneca, Genentech/Roche, MSD, BeiGene, IQVIA, Ipsen, F. Hoffmann-La Roche Ltd
Antonio Gasbarrini
Honoraria: AbbVie, Actial, Alfasigma, Eisai, Gilead Sciences, MSD, Sandoz, Sanofi, Takeda
Consulting or Advisory Role: Alfasigma, Actial, MSD, Gilead Sciences, Takeda, AbbVie
Speakers' Bureau: AbbVie
Expert Testimony: AbbVie, Alfasigma, Actial, Sanofi, MSD, Gilead Sciences, Eisai
Silvia Damian
Research Funding: Basilea Pharmaceutical
Jordi Bruix
Consulting or Advisory Role: Bayer Schering Pharma, Sirtex Medical, Novartis, Bristol Myers Squibb, Eisai, BTG, Roche, Arqule, Basilea
Speakers' Bureau: Bayer Schering Pharma
Research Funding: Bayer Schering Pharma, Ipsen
Travel, Accommodations, Expenses: Ipsen, AstraZeneca
Mitesh Borad
Stock and Other Ownership Interests: Gilead Sciences, AVEO, Intercept Pharmaceuticals, Spectrum Pharmaceuticals
Consulting or Advisory Role: G1 Therapeutics, Fujifilm, Agios, Insys Therapeutics, Novartis, ArQule, Celgene, Inspyr Therapeutics, Halozyme, Pieris Pharmaceuticals, Taiho Pharmaceutical, Immunovative Therapies, Exelixis, Lynx Group, Genentech, Western Oncolytics, Klus Pharma, De Novo Pharmaceuticals, Merck, Imvax
Research Funding: Boston Biomedical, miRNA Therapeutics, Senhwa Biosciences, MedImmune, BiolineRx, Agios, Halozyme, Celgene, Threshold Pharmaceuticals, Toray Industries, Dicerna, Sillajen, Eisai, Taiho Pharmaceutical, EMD Serono, Isis Pharmaceuticals, Incyte, Sun Biopharma, ARIAD, ImClone Systems, QED Therapeutics, Puma Biotechnology, Adaptimmune, Merck Serono, RedHill Biopharma, Basilea
Travel, Accommodations, Expenses: ArQule, Celgene, AstraZeneca
Johanna Bendell
Consulting or Advisory Role: Gilead Sciences, Genentech/Roche, Bristol Myers Squibb, Five Prime Therapeutics, Lilly, Merck, MedImmune, Celgene, EMD Serono, Taiho Pharmaceutical, Macrogenics, GlaxoSmithKline, Novartis, OncoMed, Leap Therapeutics, TG Therapeutics, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Bayer, Incyte, Apexigen, Array BioPharma, Sanofi, ARMO BioSciences, Ipsen, Merrimack, Oncogenex, FORMA Therapeutics, Arch Oncology, Prelude Therapeutics, Phoenix Biotech, Cyteir, Molecular Partners, Innate Pharma, Torque, Tizona Therapeutics Inc, Janssen, Tolero Pharmaceuticals, TD2, Amgen, Seattle Genetics, Moderna Therapeutics, Tanabe Research, Beigene, Continuum Clinical, Cerulean Pharma, Kyn Therapeutics, Bicycle Therapeutics, Relay Therapeutics, Evelo Therapeutics, Fusion Pharmaceuticals
Research Funding: Lilly, Genentech/Roche, Incyte, Gilead Sciences, Bristol Myers Squibb, Leap Therapeutics, AstraZeneca/MedImmune, Boston Biomedical, GlaxoSmithKline, Novartis, Array BioPharma, Taiho Pharmaceutical, Celgene, OncoMed, Daiichi Sankyo, Bayer, Apexigen, Kolltan Pharmaceuticals, SynDevRx, Merck, Macrogenics, Five Prime Therapeutics, EMD Serono, TG Therapeutics, Boehringer Ingelheim, Forty Seven, Stem CentRx, Onyx, Sanofi, Takeda, Abbott/AbbVie, Eisai, Celldex, Agios, ARMO BioSciences, CytomX Therapeutics, Nektar, Ipsen, Merrimack, Tarveda Therapeutics, Tyrogenex, Oncogenex, Marshall Edwards, Pieris Pharmaceuticals, Mersana, Calithera Biosciences, Blueprint Medicines, Gritstone Oncology, Evelo Therapeutics, FORMA Therapeutics, Forty Seven, EMD Serono, Merus, Jacobio, eFFECTOR Therapeutics, Novocure, Sorrento Therapeutics, Arrys Therapeutics, TRACON Pharma, Sierra Oncology, Innate Pharma, Prelude Therapeutics, Arch Oncology, Harpoon therapeutics, Phoenix Biotech, Unum Therapeutics, Vyriad, Harpoon therapeutics, Cyteir, Molecular Partners, Innate Pharma, ADC Therapeutics, Torque, Tizona Therapeutics Inc, Janssen, Amgen, BeiGene, Pfizer, Millenium Pharmaceuticals, ImClone Systems, Acerta Pharma, Rgenix, Bellicum Pharmaceuticals, Arcus Biosciences, Gossamer Bio, Seattle Genetics, Tempest Therapeutics, Shattuck Labs, Synthorx, Revolution Medicines, Bicycle Therapeutics, Zymeworks, Relay Therapeutics, Evelo Therapeutics, Scholar Rock, NGM Biopharmaceuticals, Numab, AtlasMedx, Treadwell Therapeutics, IGM, MabSpace Biosciences, Hutchison MediPharma, Repare Therapeutics, NeoImmuneTech, Regeneron, PureTech, G1 Therapeutics, Erasca Inc, Rubius Therapeutics, Pionyr, Loxo/Lilly, BioNTech AG, Elicio Therapeutics
Travel, Accommodations, Expenses: Merck, Roche/Genentech, Celgene, Daiichi Sankyo, Gilead Sciences, Bristol Myers Squibb, Lilly, MedImmune, Taiho Pharmaceutical, Novartis, OncoMed, Boehringer Ingelheim, ARMO BioSciences, Ipsen, FORMA Therapeutics
Nathan Standifer
Employment: AstraZeneca
Stock and Other Ownership Interests: AstraZeneca
Patents, Royalties, Other Intellectual Property: Patent with AstraZeneca
Philip He
Employment: AstraZeneca, Sanofi
Stock and Other Ownership Interests: Celldex, AstraZeneca, Sanofi
Mallory Makowsky
Employment: AstraZeneca
Alejandra Negro
Employment: AstraZeneca
Stock and Other Ownership Interests: AstraZeneca
Masatoshi Kudo
Honoraria: MSD, Eisai, Bayer, Lilly Japan, EA Pharma, Bristol Myers Squibb Japan
Consulting or Advisory Role: MSD, Eisai, Ono Pharmaceutical, BMS, Roche
Research Funding: Otsuka, Taiho Pharmaceutical, AbbVie, Takeda, Eisai, Gilead Sciences, EA Pharma, Sumitomo Dainippon, Ono Pharmaceutical
Ghassan K. Abou-Alfa
Consulting or Advisory Role: Silenseed, Sillajen, Agios, Bayer, Eisai, Ipsen, Merck Serono, AstraZeneca, CytomX Therapeutics, BeiGene, Genoscience Pharma, Loxo, Minapharm, QED Therapeutics, RedHill Biopharma, SOBI, twoXAR, Yiviva, Flatiron Health, Roche/Genentech, Autem Medical, Berry Genomics, Incyte, TheraBionic, Vector Health, Helio, Alnylam, Adicet Bio, Exelixis, Legend Biotech, Nerviano Medical Sciences, Surface Oncology, Yiviva
Research Funding: Bayer, Exelixis, CASI Pharmaceuticals, AstraZeneca, Bristol Myers Squibb, Incyte, Agios, Polaris, Puma Biotechnology, QED Therapeutics
Travel, Accommodations, Expenses: Polaris
No other potential conflicts of interest were reported.
DISCLAIMER
The sponsor (AstraZeneca) designed the study in collaboration with members of the trial steering committee. Data were collected by each study site and submitted to the sponsor for analysis. The sponsor collaborated with the academic authors regarding data interpretation and writing of the report. All authors had access to study data. The corresponding author had final responsibility for the decision to submit for publication.
PRIOR PRESENTATION
Presented at the 2020 ASCO Annual Meeting (Virtual), May 29-31, 2020, and the 2020 Annual ESMO World Congress on Gastrointestinal Cancer Meeting (Virtual), July 1-4, 2020.
SUPPORT
Supported by AstraZeneca.
CLINICAL TRIAL INFORMATION
VSports app下载 - DATA SHARING STATEMENT
A data sharing statement provided by the authors is available with this article at DOI https://doi.org/10.1200/JCO.20.03555.
AUTHOR CONTRIBUTIONS
Conception and design: Bruno Sangro, Ho Yeong Lim, Ann-Lii Cheng, Nathan Standifer, Philip He, Mallory Makowsky, Alejandra Negro, Ghassan K. Abou-Alfa
Administrative support: Ghassan K. Abou-Alfa
Provision of study materials or patients: William Harris, Masafumi Ikeda, Yoon-Koo Kang, Shukui Qin, Ho Yeong Lim, Wei-Peng Yong, Ann-Lii Cheng, Mitesh Borad, Masatoshi Kudo, Ghassan K. Abou-Alfa
Collection and assembly of data: William Harris, Masafumi Ikeda, Takuji Okusaka, Yoon-Koo Kang, Shukui Qin, David W.-M. Tai, Ho Yeong Lim, Thomas Yau, Wei-Peng Yong, Ann-Lii Cheng, Antonio Gasbarrini, Silvia Damian, Jordi Bruix, Mitesh Borad, Johanna Bendell, Nathan Standifer, Mallory Makowsky, Alejandra Negro, Masatoshi Kudo, Ghassan K. Abou-Alfa
Data analysis and interpretation: Robin Kate Kelley, Bruno Sangro, William Harris, Masafumi Ikeda, Takuji Okusaka, Yoon-Koo Kang, David W.-M. Tai, Ho Yeong Lim, Thomas Yau, Wei-Peng Yong, Ann-Lii Cheng, Silvia Damian, Jordi Bruix, Mitesh Borad, Tae-You Kim, Nathan Standifer, Philip He, Mallory Makowsky, Alejandra Negro, Masatoshi Kudo, Ghassan K. Abou-Alfa
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: Randomized Expansion of a Phase I/II Study
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Robin Kate Kelley
Consulting or Advisory Role: Agios, AstraZeneca, Bristol Myers Squibb, Genentech/Roche, Merck, Gilead Sciences, Exact Sciences
Research Funding: Lilly, Exelixis, Novartis, Bristol Myers Squibb, MedImmune, Merck Sharp & Dohme, Agios, AstraZeneca, Adaptimmune, Taiho Pharmaceutical, Bayer, QED Therapeutics, EMD Serono, Partner Therapeutics, Genentech/Roche
Travel, Accommodations, Expenses: Ipsen
Bruno Sangro
Consulting or Advisory Role: Bristol Myers Squibb, AstraZeneca, Bayer, Adaptimmune, Sirtex Medical, BTG, Merck, H3 Biomedicine, Ipsen, Lilly, Roche/Genentech, Eisai, Incyte
Speakers' Bureau: Bristol Myers Squibb, Bayer, Sirtex Medical, Ipsen, Lilly, AstraZeneca, Eisai, Incyte, Roche
Research Funding: Bristol Myers Squibb, Sirtex Medical
Travel, Accommodations, Expenses: AstraZeneca, Bristol Myers Squibb, Sirtex Medical, Bayer
Other Relationship: Medscape, Target Pharmasolutions
William Harris
Consulting or Advisory Role: Neo Therma, Eisai, Exelixis, Bristol Myers Squibb, QED Therapeutics, Zymeworks
Research Funding: ArQule, Exelixis, Halozyme, Bristol Myers Squibb, MedImmune, Agios, Bayer, Merck, BTG
Travel, Accommodations, Expenses: Eisai
Masafumi Ikeda
Honoraria: Taiho Pharmaceutical, Bayer Yakuhin, Eisai, Lilly Japan, Dainippon Sumitomo Pharma, Teijin Pharma, EA Pharma, MSD, Mylan, Otsuka, Yakult Pharmaceutical, Servier, Astellas Pharma, Chugai Pharma, Takeda, AstraZeneca, Novartis, Bristol Myers Squibb
Consulting or Advisory Role: Bayer Yakuhin, Eisai, Novartis, Lilly Japan, Chugai Pharma, Micron, Ono Pharmaceutical, AstraZeneca, Servier, Takeda, GlaxoSmithKline, EMD Serono
Research Funding: Bayer Yakuhin, Yakult Pharmaceutical, Lilly Japan, Ono Pharmaceutical, Eisai, AstraZeneca, Chugai Pharma, Bristol Myers Squibb, ASLAN Pharmaceuticals, Novartis, MSD, J-Pharma, Takeda, Pfizer, Nobelpharma, Merck, Delta-Fly Pharma, Chiome Bioscience, Merus NV
Takuji Okusaka
Honoraria: Eisai, Ono Pharmaceutical, Taiho Pharmaceutical, Lilly, AstraZeneca, Chugai Pharma, Yakut Honsha, Daiichi Sankyo
Consulting or Advisory Role: Taiho Pharmaceutical, Dainippon Sumitomo Pharma, Bristol Myers Squibb, AstraZeneca, Eisai, Nihon Servier
Research Funding: Novartis, Eisai, Dainippon Sumitomo Pharma, Baxter, Lilly, Taiho Pharmaceutical, AstraZeneca, Chugai Pharma, Bristol Myers Squibb, MSD
Yoon-Koo Kang
Consulting or Advisory Role: DAE HWA Pharmaceutical, Bristol Myers Squibb, Zymeworks, ALX Oncology, Amgen, Novartis, Macrogenics, Surface Oncology, Blueprint Medicines
David W.-M. Tai
Honoraria: Bristol Myers Squibb, Eisai
Consulting or Advisory Role: Bristol Myers Squibb, Eisai
Speakers' Bureau: Ipsen, Bristol Myers Squibb, Eisai, Roche
Research Funding: Bristol Myers Squibb, Sirtex Medical, Novartis
Ho Yeong Lim
Honoraria: Bayer, Eisai, MSD Oncology, Bristol Myers Squibb/Medarex, AstraZeneca
Consulting or Advisory Role: Bayer, Eisai, Bristol Myers Squibb, AstraZeneca
Speakers' Bureau: Bayer
Thomas Yau
Honoraria: Bristol Myers Squibb, MSD Oncology, AstraZeneca
Consulting or Advisory Role: Bristol Myers Squibb
Wei-Peng Yong
Consulting or Advisory Role: AbbVie/Genentech, Amgen, Bristol Myers Squibb, Ipsen, Novartis, AstraZeneca
Speakers' Bureau: Lilly, Sanofi/Aventis, Taiho Pharmaceutical, Eisai, Bayer, MSD Oncology
Travel, Accommodations, Expenses: Pfizer
Ann-Lii Cheng
Honoraria: Bayer Yakuhin, AstraZeneca, Eisai, Genentech/Roche
Consulting or Advisory Role: Bristol Myers Squibb, Bayer Schering Pharma, Eisai, Ono Pharmaceutical, AstraZeneca, Genentech/Roche, MSD, BeiGene, IQVIA, Ipsen, F. Hoffmann-La Roche Ltd
Antonio Gasbarrini
Honoraria: AbbVie, Actial, Alfasigma, Eisai, Gilead Sciences, MSD, Sandoz, Sanofi, Takeda
Consulting or Advisory Role: Alfasigma, Actial, MSD, Gilead Sciences, Takeda, AbbVie
Speakers' Bureau: AbbVie
Expert Testimony: AbbVie, Alfasigma, Actial, Sanofi, MSD, Gilead Sciences, Eisai
Silvia Damian
Research Funding: Basilea Pharmaceutical
Jordi Bruix
Consulting or Advisory Role: Bayer Schering Pharma, Sirtex Medical, Novartis, Bristol Myers Squibb, Eisai, BTG, Roche, Arqule, Basilea
Speakers' Bureau: Bayer Schering Pharma
Research Funding: Bayer Schering Pharma, Ipsen
Travel, Accommodations, Expenses: Ipsen, AstraZeneca
Mitesh Borad
Stock and Other Ownership Interests: Gilead Sciences, AVEO, Intercept Pharmaceuticals, Spectrum Pharmaceuticals
Consulting or Advisory Role: G1 Therapeutics, Fujifilm, Agios, Insys Therapeutics, Novartis, ArQule, Celgene, Inspyr Therapeutics, Halozyme, Pieris Pharmaceuticals, Taiho Pharmaceutical, Immunovative Therapies, Exelixis, Lynx Group, Genentech, Western Oncolytics, Klus Pharma, De Novo Pharmaceuticals, Merck, Imvax
Research Funding: Boston Biomedical, miRNA Therapeutics, Senhwa Biosciences, MedImmune, BiolineRx, Agios, Halozyme, Celgene, Threshold Pharmaceuticals, Toray Industries, Dicerna, Sillajen, Eisai, Taiho Pharmaceutical, EMD Serono, Isis Pharmaceuticals, Incyte, Sun Biopharma, ARIAD, ImClone Systems, QED Therapeutics, Puma Biotechnology, Adaptimmune, Merck Serono, RedHill Biopharma, Basilea
Travel, Accommodations, Expenses: ArQule, Celgene, AstraZeneca
Johanna Bendell
Consulting or Advisory Role: Gilead Sciences, Genentech/Roche, Bristol Myers Squibb, Five Prime Therapeutics, Lilly, Merck, MedImmune, Celgene, EMD Serono, Taiho Pharmaceutical, Macrogenics, GlaxoSmithKline, Novartis, OncoMed, Leap Therapeutics, TG Therapeutics, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Bayer, Incyte, Apexigen, Array BioPharma, Sanofi, ARMO BioSciences, Ipsen, Merrimack, Oncogenex, FORMA Therapeutics, Arch Oncology, Prelude Therapeutics, Phoenix Biotech, Cyteir, Molecular Partners, Innate Pharma, Torque, Tizona Therapeutics Inc, Janssen, Tolero Pharmaceuticals, TD2, Amgen, Seattle Genetics, Moderna Therapeutics, Tanabe Research, Beigene, Continuum Clinical, Cerulean Pharma, Kyn Therapeutics, Bicycle Therapeutics, Relay Therapeutics, Evelo Therapeutics, Fusion Pharmaceuticals
Research Funding: Lilly, Genentech/Roche, Incyte, Gilead Sciences, Bristol Myers Squibb, Leap Therapeutics, AstraZeneca/MedImmune, Boston Biomedical, GlaxoSmithKline, Novartis, Array BioPharma, Taiho Pharmaceutical, Celgene, OncoMed, Daiichi Sankyo, Bayer, Apexigen, Kolltan Pharmaceuticals, SynDevRx, Merck, Macrogenics, Five Prime Therapeutics, EMD Serono, TG Therapeutics, Boehringer Ingelheim, Forty Seven, Stem CentRx, Onyx, Sanofi, Takeda, Abbott/AbbVie, Eisai, Celldex, Agios, ARMO BioSciences, CytomX Therapeutics, Nektar, Ipsen, Merrimack, Tarveda Therapeutics, Tyrogenex, Oncogenex, Marshall Edwards, Pieris Pharmaceuticals, Mersana, Calithera Biosciences, Blueprint Medicines, Gritstone Oncology, Evelo Therapeutics, FORMA Therapeutics, Forty Seven, EMD Serono, Merus, Jacobio, eFFECTOR Therapeutics, Novocure, Sorrento Therapeutics, Arrys Therapeutics, TRACON Pharma, Sierra Oncology, Innate Pharma, Prelude Therapeutics, Arch Oncology, Harpoon therapeutics, Phoenix Biotech, Unum Therapeutics, Vyriad, Harpoon therapeutics, Cyteir, Molecular Partners, Innate Pharma, ADC Therapeutics, Torque, Tizona Therapeutics Inc, Janssen, Amgen, BeiGene, Pfizer, Millenium Pharmaceuticals, ImClone Systems, Acerta Pharma, Rgenix, Bellicum Pharmaceuticals, Arcus Biosciences, Gossamer Bio, Seattle Genetics, Tempest Therapeutics, Shattuck Labs, Synthorx, Revolution Medicines, Bicycle Therapeutics, Zymeworks, Relay Therapeutics, Evelo Therapeutics, Scholar Rock, NGM Biopharmaceuticals, Numab, AtlasMedx, Treadwell Therapeutics, IGM, MabSpace Biosciences, Hutchison MediPharma, Repare Therapeutics, NeoImmuneTech, Regeneron, PureTech, G1 Therapeutics, Erasca Inc, Rubius Therapeutics, Pionyr, Loxo/Lilly, BioNTech AG, Elicio Therapeutics
Travel, Accommodations, Expenses: Merck, Roche/Genentech, Celgene, Daiichi Sankyo, Gilead Sciences, Bristol Myers Squibb, Lilly, MedImmune, Taiho Pharmaceutical, Novartis, OncoMed, Boehringer Ingelheim, ARMO BioSciences, Ipsen, FORMA Therapeutics
Nathan Standifer
Employment: AstraZeneca
Stock and Other Ownership Interests: AstraZeneca
Patents, Royalties, Other Intellectual Property: Patent with AstraZeneca
Philip He
Employment: AstraZeneca, Sanofi
Stock and Other Ownership Interests: Celldex, AstraZeneca, Sanofi
Mallory Makowsky
Employment: AstraZeneca
Alejandra Negro
Employment: AstraZeneca
Stock and Other Ownership Interests: AstraZeneca
Masatoshi Kudo
Honoraria: MSD, Eisai, Bayer, Lilly Japan, EA Pharma, Bristol Myers Squibb Japan
Consulting or Advisory Role: MSD, Eisai, Ono Pharmaceutical, BMS, Roche
Research Funding: Otsuka, Taiho Pharmaceutical, AbbVie, Takeda, Eisai, Gilead Sciences, EA Pharma, Sumitomo Dainippon, Ono Pharmaceutical
Ghassan K. Abou-Alfa
Consulting or Advisory Role: Silenseed, Sillajen, Agios, Bayer, Eisai, Ipsen, Merck Serono, AstraZeneca, CytomX Therapeutics, BeiGene, Genoscience Pharma, Loxo, Minapharm, QED Therapeutics, RedHill Biopharma, SOBI, twoXAR, Yiviva, Flatiron Health, Roche/Genentech, Autem Medical, Berry Genomics, Incyte, TheraBionic, Vector Health, Helio, Alnylam, Adicet Bio, Exelixis, Legend Biotech, Nerviano Medical Sciences, Surface Oncology, Yiviva
Research Funding: Bayer, Exelixis, CASI Pharmaceuticals, AstraZeneca, Bristol Myers Squibb, Incyte, Agios, Polaris, Puma Biotechnology, QED Therapeutics
Travel, Accommodations, Expenses: Polaris
No other potential conflicts of interest were reported.
REFERENCES
- 1.Llovet JM Ricci S Mazzaferro V, et al. : Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 359:378-390, 2008 [DOI] [PubMed] [Google Scholar]
- 2.Cheng AL Kang YK Chen Z, et al. : Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 10:25-34, 2009 ["V体育官网" DOI] [PubMed] [Google Scholar]
- 3.Kudo M Finn RS Qin S, et al. : Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 391:1163-1173, 2018 [DOI (VSports注册入口)] [PubMed] [Google Scholar]
- 4.Finn RS Qin S Ikeda M, et al. : Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med 382:1894-1905, 2020 [DOI] [PubMed] [Google Scholar]
- 5.Keenan BP, Fong L, Kelley RK: Immunotherapy in hepatocellular carcinoma: The complex interface between inflammation, fibrosis, and the immune response. J Immunother Cancer 7:267, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Buchbinder EI, Desai A: CTLA-4 and PD-1 pathways: Similarities, differences, and implications of their inhibition. Am J Clin Oncol 39:98-106, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hellmann MD Ott PA Zugazagoitia J, et al. : Nivolumab (nivo) ± ipilimumab (ipi) in advanced small-cell lung cancer (SCLC): First report of a randomized expansion cohort from CheckMate 032. J Clin Oncol 35, 2017(abstr 8503) [Google Scholar (VSports注册入口)]
- 8.Naumann R Oaknin A Meyer T, et al. : Efficacy and safety of nivolumab (nivo) + ipilimumab (ipi) in patients (pts) with recurrent/metastatic (R/M) cervical cancer: Results from CheckMate 358. Ann Oncol 30, 2019(abstr LBA62) [Google Scholar]
- 9.Sharma P Siefker-Radtke A de Braud F, et al. : Nivolumab alone and with ipilimumab in previously treated metastatic urothelial carcinoma: CheckMate 032 nivolumab 1 mg/kg plus ipilimumab 3 mg/kg expansion cohort results. J Clin Oncol 37:1608-1616, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Janjigian YY Bendell J Calvo E, et al. : CheckMate-032 study: Efficacy and safety of nivolumab and nivolumab plus ipilimumab in patients with metastatic esophagogastric cancer. J Clin Oncol 36:2836-2844, 2018 ["VSports在线直播" DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Weber JS, Kahler KC, Hauschild A: Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol 30:2691-2697, 2012 [DOI] [PubMed] [Google Scholar]
- 12.Ribas A Camacho LH Lopez-Berestein G, et al. : Antitumor activity in melanoma and anti-self responses in a phase I trial with the anti-cytotoxic T lymphocyte-associated antigen 4 monoclonal antibody CP-675,206. J Clin Oncol 23:8968-8977, 2005 ["V体育安卓版" DOI] [PubMed] [Google Scholar]
- 13.Eroglu Z Kim DW Wang X, et al. : Long term survival with cytotoxic T lymphocyte-associated antigen 4 blockade using tremelimumab. Eur J Cancer 51:2689-2697, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Antonia S Goldberg SB Balmanoukian A, et al. : Safety and antitumour activity of durvalumab plus tremelimumab in non-small cell lung cancer: A multicentre, phase 1b study. Lancet Oncol 17:299-308, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.De Souza P Malczewski A Proscurshim I, et al. : Evaluation of peripheral T cell subset proliferation as a pharmacodynamic assay to guide the development of anti-CTLA-4 and PD-1 antibody combinations in patients with solid tumors. Cancer Res 78, 2018(abstr CT104) [V体育官网 - Google Scholar]
- 16.Kelley RK Abou-Alfa GK Bendell JC, et al. : Phase I/II study of durvalumab and tremelimumab in patients with unresectable hepatocellular carcinoma (HCC): Phase I safety and efficacy analyses. J Clin Oncol 35, 2017(abstr 4073) [Google Scholar]
- 17.Bruix J Sherman M; American Association for the Study of Liver Diseases : Management of hepatocellular carcinoma: An update. Hepatology 53:1020-1022, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Heimbach JK Kulik LM Finn RS, et al. : AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 67:358-380, 2018 ["V体育2025版" DOI] [PubMed] [Google Scholar]
- 19.El-Khoueiry AB Sangro B Yau T, et al. : Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 389:2492-2502, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Finn RS Ryoo BY Merle P, et al. : Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: A randomized, double-blind, phase III trial. J Clin Oncol 38:193-202, 2020 [DOI] [PubMed] [Google Scholar]
- 21.Yau T Park JW Finn RS, et al. : Checkmate 459: A randomized, multi-center phase 3 study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (PTS) with advanced hepatocellular carcinoma (AHCC). Presented at the European Society of Medical Oncology Congress, Barcelona, Spain, September 27-October 1, 2019 (abstr 6572)
- 22.Zhu AX Finn RS Edeline J, et al. : Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol 19:940-952, 2018 [DOI] [PubMed] [Google Scholar]
- 23.Hellmann MD Ciuleanu TE Pluzanski A, et al. : Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med 378:2093-2104, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Motzer RJ Tannir NM McDermott DF, et al. : Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med 378:1277-1290, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wolchok JD, Rollin L, Larkin J: Nivolumab and ipilimumab in advanced melanoma. N Engl J Med 377:2503-2504, 2017 ["V体育平台登录" DOI] [PubMed] [Google Scholar]
- 26.Yau T Kang YK Kim TY, et al. : Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: The CheckMate 040 randomized clinical trial. JAMA Oncol 6:e204564, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.El-Khoueiry A Hsu C Kang Y-K, et al. : Safety profile of nivolumab plus ipilimumab combination therapy in patients with advanced hepatocellular carcinoma in the CheckMate 040 study. Presented at the 13th Annual Conference of the International Liver Cancer Association, Chicago, IL, September 20-22, 2019
- 28.Enrico D Paci A Chaput N, et al. : Antidrug antibodies against immune checkpoint blockers: Impairment of drug efficacy or indication of immune activation? Clin Cancer Res 26:787-792, 2020 [DOI] [PubMed] [Google Scholar]
- 29.Davda J Declerck P Hu-Lieskovan S, et al. : Immunogenicity of immunomodulatory, antibody-based, oncology therapeutics. J Immunother Cancer 7:105, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.TECENTRIQ (Atezolizumab) Injection: [Highlights of Prescribing Information]. South San Francisco, CA, Genentech, 2020. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761034s009lbl.pdf [Google Scholar]
- 31.OPDIVO (Nivolumab) Injection: [Highlights of prescribing Information]. Princeton, NJ, Bistol Meyers Squibb, 2020. https://packageinserts.bms.com/pi/pi_opdivo.pdf [Google Scholar]
- 32.Das R Verma R Sznol M, et al. : Combination therapy with anti-CTLA-4 and anti-PD-1 leads to distinct immunologic changes in vivo. J Immunol 194:950-959, 2015 ["V体育安卓版" DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sangro B Gomez-Martin C de la Mata M, et al. : A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J Hepatol 59:81-88, 2013 [DOI] [PubMed] [Google Scholar]
- 34.Bruix J, da Fonseca LG, Reig M: Insights into the success and failure of systemic therapy for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol 16:617-630, 2019 ["V体育平台登录" DOI] [PubMed] [Google Scholar]
- 35.Reig M Rimola J Torres F, et al. : Postprogression survival of patients with advanced hepatocellular carcinoma: Rationale for second-line trial design. Hepatology 58:2023-2031, 2013 [DOI (VSports)] [PubMed] [Google Scholar]
- 36.Wolchok JD Hoos A O'Day S, et al. : Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin Cancer Res 15:7412-7420, 2009 [DOI] [PubMed] [Google Scholar]
- 37.Hodi FS Hwu WJ Kefford R, et al. : Evaluation of immune-related response criteria and RECIST v1.1 in patients with advanced melanoma treated with pembrolizumab. J Clin Oncol 34:1510-1517, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mamdani H Wu H O'Neil BH, et al. : Excellent response to anti-PD-1 therapy in a patient with hepatocellular carcinoma: Case report and review of literature. Discov Med 23:331-336, 2017 [PubMed] [Google Scholar]
- 39.Pennock GK, Waterfield W, Wolchok JD: Patient responses to ipilimumab, a novel immunopotentiator for metastatic melanoma: How different are these from conventional treatment responses? Am J Clin Oncol 35:606-611, 2012 [DOI] [PubMed] [Google Scholar]
- 40.Shimomura A Fujiwara Y Kondo S, et al. : Tremelimumab-associated tumor regression following after initial progression: Two case reports. Immunotherapy 8:9-15, 2016 [DOI] [PubMed] [Google Scholar]
- 41.Assi H, Wilson KS: Immune toxicities and long remission duration after ipilimumab therapy for metastatic melanoma: Two illustrative cases. Curr Oncol 20:e165-e169, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pires da Silva I Lo S Quek C, et al. : Site-specific response patterns, pseudoprogression, and acquired resistance in patients with melanoma treated with ipilimumab combined with anti-PD-1 therapy. Cancer 126:86-97, 2020 [DOI] [PubMed] [Google Scholar]
- 43.Wilgenhof S Du Four S Everaert H, et al. : Patterns of response in patients with pretreated metastatic melanoma who received ipilimumab 3 mg/kg in a European expanded access program: Five illustrative case reports. Cancer Invest 30:712-720, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hoos A Wolchok JD Humphrey RW, et al. : CCR 20th anniversary commentary: Immune-related response criteria—Capturing clinical activity in immuno-oncology. Clin Cancer Res 21:4989-4991, 2015 [DOI] [PubMed] [Google Scholar]
- 45.Edeline J Karwal M Zhu AX, et al. : RECIST v1.1 and irRECIST outcomes in advanced HCC treated with pembrolizumab (pembro). J Clin Oncol 38, 2020(abstr 528) [Google Scholar]
- 46.Zimmermann S, Peters S: Appraising the tail of the survival curve in the era of PD-1/PD-L1 checkpoint blockade. JAMA Oncol 5:1403-1405, 2019 [DOI] [PubMed] [Google Scholar]
- 47.Ferrara R Pilotto S Caccese M, et al. : Do immune checkpoint inhibitors need new studies methodology? J Thorac Dis 10:S1564-S1580, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Harris SJ Brown J Lopez J, et al. : Immuno-oncology combinations: Raising the tail of the survival curve. Cancer Biol Med 13:171-193, 2016 [V体育ios版 - DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
A data sharing statement provided by the authors is available with this article at DOI https://doi.org/10.1200/JCO.20.03555.